How to think about artificial intelligence applications like a designer: a case study

If you love your hammer, everything looks like a nail. So why not start hammering straight away? All too often in artificial intelligence, the rush to implement overtakes a fuller appreciation of the problem at hand, spawning underwhelming solutions. Here, with a worked example, we explain how to take a broader view
It’s part of human nature to see everything through the prism of our own experience. Whether you’re a writer or a physicist, this trait has its uses – but it can also lead to incomplete, siloed ideas, rather than thought-through, workable solutions, that truly address the question of: what’s the job to be done?
Artificial intelligence projects are particularly prone to tunnel vision, probably because the technology is so new and everyone is itching to unleash it. Guided by misleading metaphors, people often zero in on the first thing they see that falls within the familiar category of problems that can be addressed by algorithmic machinery. But is that the right focus? Will it truly make a difference?
AI companies often get caught up in the proof-of-concept trap, pushing promising ideas too quickly through to expensive testing stages, when taking a quick step back to consider that idea in context would have revealed its shortcomings.
A case study: when alarms cry wolf
Imagine you are working on a project that aims to optimise alarm management in hospital ICUs.
The overwhelming majority of alarms – between 72% and 99% – are actually false-positive, which means the only action required is that they be manually stopped by hospital staff.
As the multitude of sensors connected to patients in a modern-day ICU grows, this high incidence of false-positives becomes an ever more pressing problem. Patient safety is undoubtedly enhanced, and the sensors enable better therapy – but the daily flood of alarms can desensitize hospital staff, eventually causing alarm fatigue.
How might artificial intelligence mitigate this problem?
Well, surely that’s pretty clear? Deciding alarm vs no-alarm, based on sensor data, is a good-old classification problem, which is what machine learning is all about (kind of). So let’s dust off the random forests and the neural networks and get cracking, right?
Wrong. Now is the time to take the blinkers off and get a broader view. Question your fundamental assumptions. Can the situation really be best improved simply by filtering false-positive alarms? And even if so, where should the bar be set for alarm filtering success; would a 5 percentage point reduction in false-positives warrant investment? Could it be that the true value of this project lies in discovering solutions beyond the most obvious?
To find those solutions, you’ll need to think like a designer rather than an implementer: go broad before you go deep and embrace discovery first. Embrace the ambiguity, embrace the complexity. If you stop at the first sight of something that looks like it can be addressed by an algorithm, you’ll have missed your chance to fully understand the situation.

AI-enabled solutions are hard to envision. The familiar tactics for rapid prototyping to validate, invalidate and iterate a potential solution are not so effective in an area where the core is so abstract. And this makes it hard to even talk about them.
A design approach to artificial intelligence
AI-enabled solutions are hard to envision. The familiar tactics for rapid prototyping to validate, invalidate and iterate a potential solution are not so effective in an area where the core is so abstract. And this makes it hard to even talk about them.
However, the first lesson to take from design is that the research phase must be seriously considered, and approached in a structured way. Don’t even think about data and algorithms before you’ve invested a good chunk of time – at least two weeks of proper research – into getting to know the broader environment your AI project will sit within inside-out. Research done, it’s time to structure the problem space; here’s how we do it …
Step 1: Getting the big picture into view
Mind maps are simple but effective tools. Put your topic – in this case ‘Alarm management in the ICU’ – at the centre and record whatever associations spring to mind around it – from adjectives to objects, people and processes. In this example, starting with free associations might yield words such as loud, confusing or patient information. Thinking precisely about processes might generate words such as alarm confirmation, prioritisation or conclusion (for therapy).

Step 2: Put some structure on it
The next step is to review your mind map and start grouping associations into clusters. These will help you structure your thoughts and think more efficiently about the project’s topic and its underlying connections. Then name your clusters. This will help you identify other fields that may be relevant to those clusters.

Step 3: From clusters to levers
Next up, you’ll want to identify some levers: factors that can be directly influenced by the potential AI application. Meticulously thinking through “insight-to-action” or “prediction-to-action” is one of the crucial steps that is often overlooked. To do this, look at each individual cluster in turn. Is it something that could directly be improved through your work? If not, is there a related aspect the project could influence? Again, free your mind from the tyranny of the familiar machine learning toolbox! More often than not, there are indirect routes for algorithms to have an impact.
In our example, the Shortage of staff cluster is not something you can directly influence using data science. Workload Management, however, is; algorithms could “intelligently” divide and assign alarms only to certain staff, for example, lightening others’ workloads.
Therefore, you would derive the Workload Management lever from the Shortage of staff cluster.

Another example could be the layout of the rooms in an ICU – relevant because inconvenient room layouts can lead to staff taking circuitous routes and alarms going off for longer, putting patients at greater risk.
Since you are not an architect, you cannot influence the layout of rooms – but what you can influence is which routes are taken by whom (by, for example, using algorithms to suggest an order in which alarms should be processed to optimize the routes taken by the staff).
Therefore, you derive the lever Workflow Optimization from the Room Layout cluster.
Step 4: Pulling the levers
Now you’ve identified all the levers you can influence, you should be able to devise a range of more complete solutions. And you can always add up to your topics later on, by repeating steps 1 to 3 or by adding relevant subjects as they crop up.
Just make sure everything you add to your map brings more clarity (not more complexity) and is relevant to your work. By the end of the exercise you’ll have defined a broad range of situations that are ripe for improvement. In the ICU example, we identified five key levers.
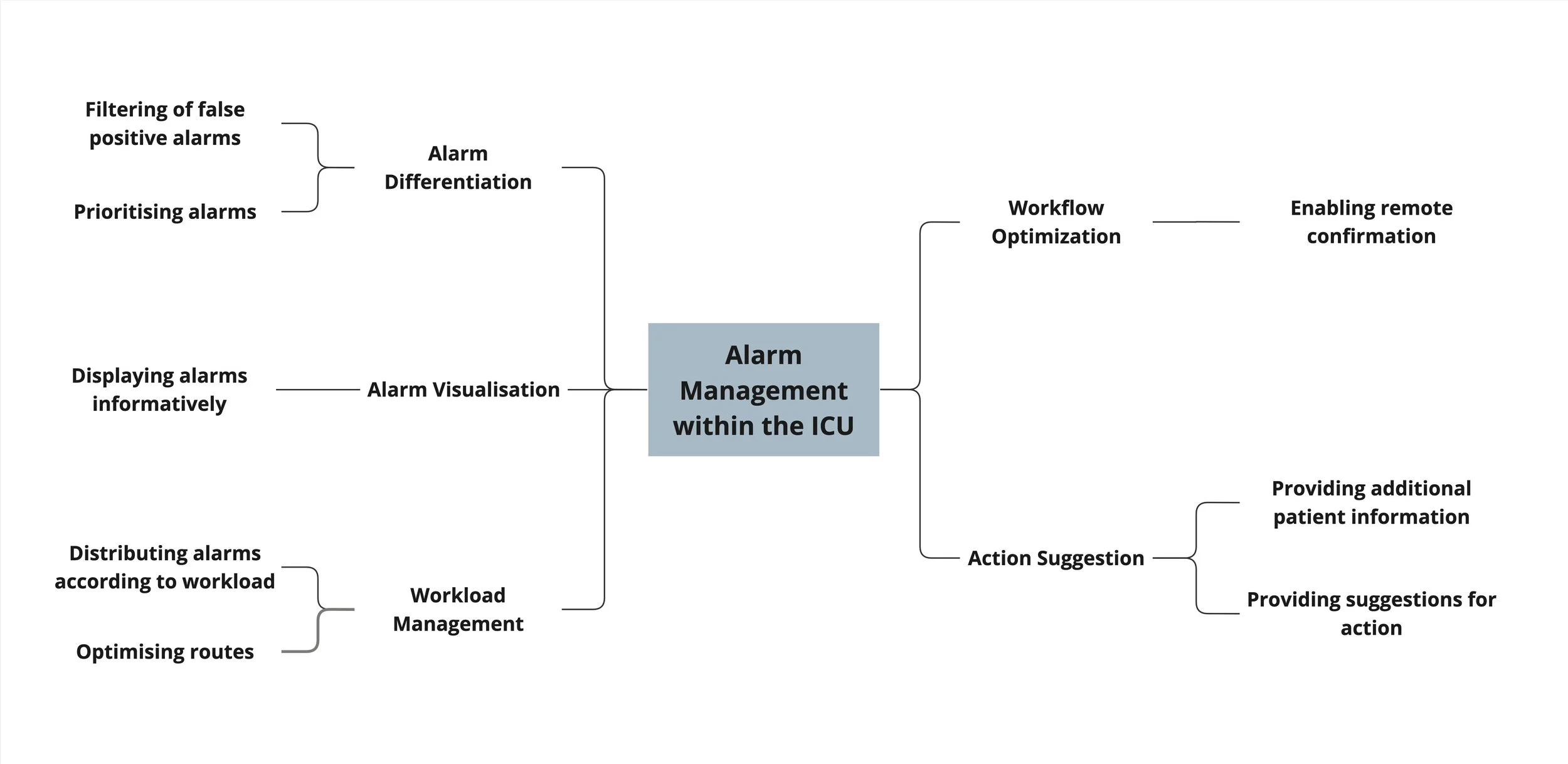
Lever “Alarm differentiation”. Instead of simply seeking to reduce the frequency of alarms, we could use algorithms to prioritise them. Medical staff might then only need to interact with top-priority cases. This approach would still carry a risk – of a genuine emergency being downgraded. And yet the repercussions would be less than in the naive binary approach, where that alarm would never even have been triggered.
Lever “Informative alarm displays”. If the aim of an alarm in the ICU is to inform medical staff that a patient’s therapy is not going as planned, those alarms should tell you everything you need to know. Simple sirens tell you very little. Variations in sound (frequency and tone) and light (colour and intensity) could indicate different types or severities of alarm, helping staff interpret the situation and draw swifter conclusions.
Lever “Workload management”. Staffing levels vary between hospitals and even between shifts in the same hospital, which can make even distribution of duties difficult. If staff could be assigned responsibility for these alarms according to their current workload, and provided with a route that helps them move from A to B (and C and D perhaps) to deal with them more efficiently, this capacity problem would be mitigated.
Lever “Workflow optimization”. And what if staff didn’t need to physically move to where that alarm is going off to confirm it? Given the vastness of modern hospitals, the remote confirmation of alarms promises sizeable reductions in time and effort – plus the technology is relatively simple and easy to integrate into medical staff’s working lives.
Lever “Action suggestion”. Finally, what if an alarm did more than alerted medical staff to the situation? Typically, staff responding to an alarm see just a headline and a short description stating the circumstance that set it off. They then have to analyze what exactly caused the alarm, as the culprit can be a combination of different patient parameter values, fed via different machines, plus sensor or machine failure. Only after this often time-consuming and confusing task can they suggest a suitable change of response.
Step 5: Comparing your options
These are all good options – the question is which one should we do first? Again, think breadth. Before diving deep into any one option – or all of them (which would be a hell lot of work) – let’s assess each one along three dimensions:
Barriers to acceptance: how easy will it be to fit the solution into the existing workflows – and minds – of hospital staff?
Mode of intervention: will the solution provide staff with extra information, or recommend further action (or both)?
Technical complexity: how difficult will it be to implement and integrate?

The obvious quick-win is providing better alarm visualization. Low tech complexity and straightforward integration make it an obvious first step that would quickly improve the situation. Remote alarm confirmation would also be technically quite simple – although hospitals and their staff may be uneasy about introducing a system that did not require a patient visit for each alarm.
Next up in terms of feasibility are the interventions that recommend actions, such as how responsibility for alarms is assigned to staff and optimising the route they take to deal with them in the most efficient way.
Ultimately, it all depends on the exact nature of the challenge you’re facing. If the root cause seems to be a very imprecise alarm system, then running a proof-of-concept to see whether you can get more relevant alarms, either by suppression or prioritisation, makes absolute sense. Once that option is exhausted, however – or if it’s not the key issue – workload management assistance is the way to go.
If you want to learn more about how to approach innovation with artificial intelligence in a structured way, get in touch. We are happy to walk you through how we develop and validate a proper concept before embarking on a proof-of-concept implementation.
Further reading
7 Ways to Get Started Designing for AI/ML Products (Lola Salehu) makes that case for shaping your algorithm with design decisions, not the other way around – using concrete examples of where this went wrong.
A new study shows what it might take to make AI useful in health care (Karen Hao, MIT Technology Review) argues that barriers to collaboration between ML/AI researchers and clinical practitioners need to come down for this new technology to have a positive impact for patients.
The proof of the pudding: in praise of a culture of real-world validation for medical artificial intelligence (Federico Cabitza and Jean-David Zeitoun, Annals of Translational medicine) shows how validation of AI use cases must go far beyond the statistical: relational, pragmatic, and ecological validity are essential.